
This post may contain affiliate links. As an Amazon Associate, I earn from qualifying purchases.
My painful and scary experience with post operative ileus complications left me very weak, under 100 pounds, malnourished, and very close to death’s door
My post-surgery complications started with pancreatitis and then after my ileostomy takedown surgery, morphed into multiple battles with post operative ileus.
Table of Contents
- Emergency Room
- NG (Nasogastric) Tube
- Hospital Room
- Getting the NG Tube Out
- Discharge Process
- Getting Home
- Emergency Room and Hospitalization
- X-Rays
- Second NG (Nasogastric) Tube Experience
- Pouchoscopy
- Endoscopy
- Getting Antsy, Impatient, and Frustrated
- Deep Vein Thrombosis (DVT)
Yes, it’s possible to die from ulcerative colitis
Weaknesses in the medical care system
Recovering from Pain and Standing in the Sun
Hospitalizations
- Pancreatitis: 3 days, August 15th – 17th
- Ileostomy Takedown Surgery: 3 days, August 30th – September 1st
- Post Operative Ileus Round #1: 6 days, September 2nd – 7th
- Post Operative Ileus Round #2: 11 days, September 25th – October 5th
Total Days: 23

In Part XIV – Ileostomy Takedown Surgery I wrote about my small but big surgery in Antioch on Tuesday, August 30th. I left off on how I woke up the morning of Friday, September 2 vomiting, which is never a good sign after surgery.
That was the beginning of my brutal first round of post operative ileus.
Post Operative Ileus Round #1: Friday, September 2nd – Wednesday, September 7th
Early Friday morning, I woke up barfing nonstop. You use your stomach muscles when you bark and it hurt a lot because of the surgery.
My mom kept trying to get me to eat but I didn’t want anything and I was steadily feeling more and more pain.
I debated who to call for a while. In the discharge papers, there is a number listed. But it is basically just the general advice line. So first I called Antioch surgery since I had my surgery there, and I left a message with a general surgeon nurse but nothing happened.
Then I called the advice line for Vacaville Kaiser and I eventually got put in touch with a nurse. She grabbed a hold of the surgeon on call in the ER and he relayed that I needed to go to the ER immediately.
Emergency Room
My mom took me to the emergency room and luckily, it was extremely empty. I thought it might be really crowded because it was Friday on Labor Day weekend.
I got a room immediately, got in a gown, and had an IV line set up right away. Because I was in a lot of pain and vomiting, the nurses kept me dosed with morphine and nausea medication.
The doctor ordered an x-ray first, which showed my intestines were dilated. But he felt like he needed a better visual so I got a CT-Scan next. The CT-Scan showed there were no blockages but that my intestines weren’t working and I had a lot of fluid in my abdomen.
After that, an NG (nasogastric) tube, was ordered.
NG (Nasogastric) Tube
An NG (nasogastric) tube, is a flexible plastic tube that is passed through the nose, down the esophagus, and into the stomach. It’s then attached to a pump that removes substances from the stomach. This helps relieve the pressure and pain caused by the dilated intestines.

My nurse came into my room, sat down, and explained the procedure a couple of times because it’s one that is made easier with the patient’s cooperation.
He said about halfway through the process, my body would start having a “no” reaction. I’d start rejecting what was happening to me but he was going to keep forcing the tube down. He said I would hate him but that his forceful actions would make him my best friend.
Insertion
Prep-wise, the back of my throat was sprayed with a lemon-flavored numbing agent. The nurse put the head of my bed all the way up, so that I was sitting upright. And then he started pushing the tube up my nose.
Sure enough, at first, when the tube was going in, it didn’t feel too bad. But it gets to a certain point past your nose and suddenly, it’s horrible. That’s when my head started jerking back, trying to escape the pressure. But he forced my head forward.
Mid-throat is when there is a pause in the procedure. I had to put my chin to my throat and sip on some water while the nurse held my head down. Sipping and swallowing the water helps the tube slide down the esophagus and get into the stomach. It feels like something is trying to stab its way out of your throat.
Once the tube was in, the nurse turned on the pump and so much fluid started pumping out of me.
Having an NG tube made me feel like I had an elephant trunk for a nose. They tape it to your nose to prevent it from moving around or being pulled out.
Initially, it did start to make me feel better but I was still in a lot of pain. My nurses were giving me morphine every hour and I wasn’t even asking for it.
But eventually, I threw up with the NG tube in. And that felt horrible. I also feel like it was less effective after that. The pain started to increase again, there was a stabbing pain in my throat, and the morphine stopped working.
Hospital Room
I was hospitalized around 4 PM on Friday, September 2nd. By the time a hospital room opened up for me, my throat and abdomen started hurting very badly. I think I was at the tail end of a morphine dose when they started to transfer me.
Once I got situated on the hospital bed and hooked up to the pump again, the nurse put it on an intermittent setting. In the ER, it was pumping extremely fast, continuously. In my hospital room, it was pumping at a much slower speed with long pauses. During the pauses, I watched as fluid would flow back up the tube and into my nose.
The nurse left and said she would be right back. I hadn’t gotten any more pain meds and at this point, everything had worn off. It felt like an eternity for her to get back to my room.
Excruciating Pain
While I was waiting, I held on to both my parents’ hands, gripping onto them for dear life. I started sobbing because the pain was so bad. But that made the pain worse because there was a tube in my throat.
This was excruciating for me but also for my parents. At one point I saw my dad push his glasses up to wipe tears from his eyes. He still thinks it’s the most pain I’ve ever been in. I’ve never sobbed like that before.
It’s a pain level that defies description or categorization. I call it a pain level that is so painful, you actually need to cause pain somewhere else so that all the attention isn’t on that one area.
At one point a nurse came in a said, “That tube is too long, we need to change it.” So, she did, and I immediately started to feel better. Soon, I also got more pain medication administered, which helped a lot.
But I had to practice controlling my emotions and deep breathing because anything that caused my throat to tighten even a little made the pain worse.
Being Scared
My mom offered to stay the night with me and at first, I said no. But 10 minutes later, I changed my mind.
I couldn’t talk because of the tube down my throat and I felt more scared than normal. Ulcerative colitis stuff is an old hat. Pancreatitis sucked but once I knew what was going on, it was just something else to deal with.
But this was something different. I had never felt the need to ask somebody to stay the night with me while in the hospital before. But this time, I needed someone there with me.
She was able to communicate to the nurses and doctors for me, advocate for me when we felt like something was wrong (the NG tube), and be a steady comforting presence for me.
Getting the NG Tube Out
The NG tube was extremely annoying. To go to the bathroom or walk, I had to get a nurse to detach me from the pump. I also felt like it wasn’t working.
The pain in my throat was getting worse and worse. When you can’t drink anything or even eat ice, your skin gets incredibly dry. Your lips stick to your teeth and start to crack. My throat was extremely dry too and it felt like the tube was starting to get glued to my esophagus.
Every morning, radiologist technicians would come into my room with a portable x-ray machine and take pictures of my abdomen. And every morning, the images showed that my intestines were still dilated and not functioning.
This also has some role in helping doctors decide whether or not to remove the NG tube. The surgeon on call would come at the same time every day in the morning and ask me questions. On Sunday, September 4th, he asked if I wanted the NG tube out and I said yes.
I felt like it had done its job but that at that point, the cure was causing just as much pain as the cause. Once it was removed, I immediately began to feel better.
It also made my stay in the hospital more…hospitable. My nurses didn’t really get to know me until the NG tube came out. They would ask me questions or try talking to me but the pain was so bad it made me want to cry every time I tried to answer them.
Discharge Process
Any time I’m hospitalized, a good sign that I’m close to being better is that I get bored, antsy, and want people to visit me. Each day was getting better but I also was trying to be patient. It’s never good to rush the process.
When you have post operative ileus, to get cleared for discharge, you have to be re-introduced to liquids and solids without vomiting. The order goes:
- Clear liquids like water, apple juice, jello, and broth
- Full liquids like cream of wheat, creamy soups, pudding, and yogurt
- Solids – sometimes you will be introduced to soft solids first, like pureed food, or go straight to a full regular diet

On Tuesday, September 6th I was advanced to a full liquid diet. When I did okay with that, I was given some French toast to try on Wednesday morning. Although it tasted awful, I didn’t throw up, so I got discharged.
Getting Home
Going from hospital life to home life is always a little jarring.
You can have so much energy at the end of your hospitalization. But once you get home, all that energy disappears. Because doing laps around the hospital floor is a lot different than going back to your daily routines.
I’m always the most excited for the shower when I come home from the hospital. But this time, it was especially exciting because I hadn’t had a shower since August 29th. When I got home on September 1st, I had to settle for a sponge bath because my incision site was still oozy.
While I was hospitalized, my wound healed up enough that I got to take a shower when I got home. And it was amazing.
After weeks of dehydration and malnutrition, I weighed 100 pounds. I looked like a junky because my veins were shot. If I had to go to the ER for some reason, I don’t think they would have been able to find a vein in my body that hadn’t been poked or attached to something. I think they would have had to use a leg.
It was hard to go on my walks with my arms uncovered because of all the bruises and swelling. It made me feel very self-conscious.
I could finally eat and stuck to a low fiber and extremely low-fat diet. Although it hurt a little to eat, I wasn’t throwing up, so I felt like I was truly over the whole ordeal.
In the eye of the storm, September 8th – 24th
I think a good analogy for the period of time between round one of post operative ileus and round two, is that it was like being in the eye of the storm.
Unsuspecting sailors might not know they are in a hurricane. So, when they suddenly seem to come out of the storm, they might think the worst is over. Little do they know, they are just in the eye of the storm, and only halfway through their ordeal. I’m the unsuspecting sailor in this analogy.
One of my main obstacles during this time period was that I didn’t know how I was supposed to be feeling. My body was learning how to work in a wholly different way. How was I to know what was right or wrong?
Increasing Pain
In general, I thought I felt pretty good. I was eating healthy but it felt like I was forcing myself to eat because I knew the pain would be bad. And it got worse throughout the week. I started feeling intense cramps after eating. They were almost like a full-body seizure.
I was sent home with some Norco but I’ve always been very reluctant to take opiates outside of the hospital because they scare me.
Originally, I was only taking them at night because nights were the worse. I was only getting four hours of sleep because the stomach spasms were so bad that they kept me up.
To help, I tried changing my eating habits even more, like eating a snack sized meal every two hours. That didn’t decrease the amount of cramping, but at least the pain started early enough that by bedtime, the pain wasn’t so bad.
My reluctance to take the Norco in the end made me feel worse. Because I was in so much pain, my whole body began to hurt. My knees, elbows, wrists, and shoulders were achy and sore.
Moving was lethargic, like I was walking through a thick resistant substance. My blood pressure was the lowest it’s ever been, around 75/40. Anytime a nurse tried to take my blood pressure, alarms started ringing.
Because my j-pouch was being used for the first time and my anus was back to working order after a three-month hiatus, my butt burn was really bad. It hurt to sit and move because my skin down there was so irritated.
But ultimately, it was the stomach spasms that were taking the biggest toll on me.
Emergency Room Visit, Monday, September 12th
After surgery, you are supposed to go to the ER if you have a fever at or above 101.5, vomiting, swelling, or unmanageable pain.
My pain was very unmanageable. But I’ve found that it’s never a factor in getting admitted to the hospital. It’s not like I wanted to be admitted, but when you’re in so much pain, you want a little extra help.
Sunday, September 11th, I got a really bad heart burn feeling again, which is the symptom that preceded the throwing up and being hospitalized for post-operative ileus.
I went ahead and called the 24-hour advice line at 12:30 in the morning on Monday, September 12th. A nurse listened to my symptoms and she went directly to a doctor who said I should come in just in case.
I got an IV in, some x-rays, and pain meds. While waiting for results, I was due for another dose of Dilaudid. And I wanted it so bad.
But the nurse did a nervous laugh when she took my blood pressure and decided it was too dangerous to give me a dose. The x-rays didn’t show anything so a doctor discharged me.
I was a little disappointed. I felt like I needed help. After being discharged, I decided that I was going to have to start taking more opiate doses to get the help I needed.
Pain and Nausea Management
Because the x-rays didn’t show anything, I was trying to understand if the symptoms I was experiencing were natural after having the take down surgery or not. When I looked at forums on the topic, many people said that they had to deal with cramps a lot.
But these were just as bad or even worse than my ulcerative colitis cramping and spasms. I was having to grab onto the wall or hit something to get through them.
I began to feel worn down and hopeless, and I always felt very close to breaking down in tears because I was so done.
After I was sent home from the ER, I was prescribed Reglan, which I liked because it knocks you out. I was already taking Zofran, which you can take every 8 hours. But the doctor wanted to give me another option that I could use between Zofran doses for when I was nauseous.
After the ER visit, I gave in and began taking more Norco. I couldn’t deal with the pain anymore. However, I still wasn’t taking a lot. You can technically take a dose every 3 hours, but I took only two or three doses a day.
Opiate Addiction Fears
I never had any real fears about opiate addiction. Before 2016, my hospitalizations averaged once a year. I was only administered opiates while in the hospital, and they weaned me off before I was discharged.
But the constant hospitalizations and the unrelenting pain of 2016 meant that my exposure and dependence on opiates were greatly increased. And I began to fear I would become addicted.
My fear of opiates is not only about addiction. They can slow down your digestive track, cause abdominal cramping, and constipation. It’s a vicious sort of cycle.
You need the opiate because of the amount of pain you are in but at some point, they can also cause pain, delay recovery, and exacerbate the problems that caused the pain in the first place.
My intestines and digestive track are already fucked up enough. Extending opiate use just fucks them up more.
Post Operative Physician’s Assistant Appointment, Tuesday, September 13th
After being discharged from the ER without any answers on Monday, I was looking forward to my post operative appointment. I wanted to ask so many questions.
- Are these serious cramps and spasms normal?
- What’s the deal?
- Is this amount of pain normal?
- What can I do to help stop this?
I was very interested in what he was going to say.
Breakdown in Communication
When I was hospitalized, two different people in the Vacaville hospital told me they would update my surgeon on my condition.
And while I was in the hospital, a physician’s assistant that was supposedly part of my surgeon’s team called me for a follow-up phone appointment. Once she found out what was going on with me, she told me she would update Dr. Freshman on my condition.
With all my experience, I also know that it’s good to be your own advocate. I tried to send a message to Dr. Freshman updating him on my condition, but the Kaiser Permanente system wasn’t working properly and kept kicking me off.
I figured I was covered though. But I wasn’t. Nobody had informed him, or his team, what was going on with me. They had no idea I was in the hospital for 6 days because of post operative ileus. So, there was a breakdown in communication on multiple levels.
At the appointment, the physician’s assistant was overwhelmed with the amount of information I was throwing at him. And he was pissed. Not at me. He was very angry that he didn’t know what was happening to me during that time. And he knew Dr. Freshman was going to be angry too.
Antibiotic Treatment
The horrible intense cramps that I was feeling were not normal at all. After a series of questions and a physical examination, the physician’s assistant left the room for ten minutes. He came back saying he had talked to Dr. Freshman who ordered a C-diff test.
As soon as he mentioned that test, I was in familiar territory. A C-diff test is a stool test that rules out bacterium causes of severe diarrhea and colitis. If that test comes back negative, it usually means you are in an ulcerative colitis flare, or in this case, pouchitis.
I was prescribed the antibiotic Cipro before even taking the tests though. There was obviously something wrong with me and antibiotics are used to treat pouchitis. But I did test negative for C-diff.
Dr. Freshman wanted me to call him immediately if I was still feeling just as bad three days later. If that was the case, a CT Scan would need to happen to see if something else was causing the problems.
The antibiotics did seem to help at first, especially during the three-day time period Dr. Freshman had laid out. So, I didn’t contact him.
Feeling like a failure
At this point, I felt like I had failed a test and I doubted my future with the j-pouch. My j-pouch was already not working.
I tried to remind myself that a lot of people experience at least one case of pouchitis in their lifetime. Mine just happened right after I got my j-pouch. The light at the end of the tunnel seemed a little further away to me.
Although I initially saw some improvement, my pain was still serious, especially at night, and I felt the Norco wasn’t working as well as before. I pulled a muscle in my back from all the squirming around I was doing at night because of pain. Occasionally, I felt nauseous as well.
Post Operative Ileus Round #2: 11 days, Sunday, September 25th – Wednesday, October 5th
My second round of post operative ileus happened suddenly, like someone flicking a switch. I feel like there must have been a transition but honestly, I can’t pinpoint the change. It was BOOM-all of a sudden, I was in extreme excruciating pain.
I wasn’t nauseous though like the first time. Because I never throw up, it was easy for me to know that something was wrong. But because the pain was so intense, I called the advice line. It was 2 in the morning and I was having trouble talking because the pain was so bad.
The nurse said, “you don’t need permission to come to the ER, just come. If you have to drive yourself and have to stop, just stop and call an ambulance and they’ll come to pick you up. JUST COME IN.”
So, I woke my mom up and she got ready and took me to the ER. The pain was occupying most of my mind and body, but under it all, I was confused. I was unsure if post operative ileus could happen again once a certain time had passed after surgery.
Emergency Room and Hospitalization, Sunday September 25th
I was in an indescribable amount of pain by the time I was admitted to the ER. The bed was rattling because I was holding onto the bed railing for dear life while my body was vigorously shaking uncontrollably.
They kept giving me doses of Dilaudid every hour but it only worked for 30 minutes. I would then suffer and have to wait 30 more minutes for another dose. It was intense and I don’t remember that much.
Every time I got a dose of Dilaudid, I felt a heat come over my skin and immediately felt extremely itchy. The itchiness would last a couple of minutes and then fade. But eventually, I had permanent hive-like pimples across my neck and shoulders. This wasn’t an allergic reaction and one of my nurses said it is a less common symptom from frequent opiate use.
Around 7 in the morning my nurse did some magic tricks for me before transferring me to a hospital room. I remember that.
Once I got to my room, I took a turn for the worse. I got really bad chills and I couldn’t stop shivering. The bed began rattling again. My heart rate was very high and my blood pressure was very low.
My vision was blurry, I was in and out of consciousness, and I just remember my nurse’s face popping back in and out of focus and her saying she was really worried.
That’s all I remember for the next 3 days.
X-Rays
Eventually, I was awake and coherent enough to be given a barium contrast solution to drink. They wanted to take x-rays 8 hours and 12 hours later to get a better picture of my intestines.
I drank the solution with lots of ice because I knew that was the last water I was going to be getting for a while. My mom had to keep shaking me to keep me awake and stop me from spilling the solution.
X-ray technicians used a portable x-ray machine, so I didn’t have to go anywhere. The x-rays didn’t end up showing anything conclusive. There was no definite spot of blockage or stricture.
I started vomiting and the cramping and spasms were so bad that I was taking Dilaudid every hour.
Monday morning, I was scheduled for a kind of colonoscopy-type procedure to check out my j-pouch. But because of the vomiting, it was decided that I needed to have an NG tube inserted first.
Second NG (Nasogastric) Tube Experience, Monday September 26th

The first time I had an NG tube done, it was bad. This time was diabolical. There was projectile vomiting, choking, gagging, spewing. The list of adjectives could continue.
I wasn’t given any kind of prep this time around. No numbing spray or anything. My nurse made my dad leave the room, which I’m grateful for because it was horrible.
As the tube was going down my throat, I started to vomit and began choking on the tube and my own vomit and saliva.
The vomit was this weird rust brown-red color and it got all over me. As I was choking, I started crying and begging the nurse, asking her if she could take out the tube. Eventually, the nurse got the tube in properly.
By this time, the GI people were waiting to take me down to surgery for the scope. But they had to wait for an x-ray team to come by, so they could confirm that the tube was in the right position.
While waiting for the x-ray, a tech helped me clean up. This was probably the most vulnerable I ever felt. During all my hospitalizations, I’ve always maintained some independence when it comes to intimate tasks like bathing.
The tech took me to the bathroom and helped undress me and wipe me down while I shook like a shivering wet chiwawa. I felt like I was an outside observer to my body, watching this woman clean me like a baby.
Pouchoscopy, Monday September 26th
After the x-rays were done, I was rolled off to get a pouchoscopy, a scope of the j-pouch. This is a procedure that is done under anesthesia and I was very happy to be put out of my misery for a little while.
My j-pouch looked great, with only a small amount of inflammation. There weren’t any obstructions or strictures, which meant that surgery wasn’t going to be needed. But that meant I had to wait it out.
Over the next couple of days, pain was my companion. I don’t remember that much. The combination of pain, opiates, and nausea medicine makes memory foggy at best.
IV Nutrition, Wednesday September 28th
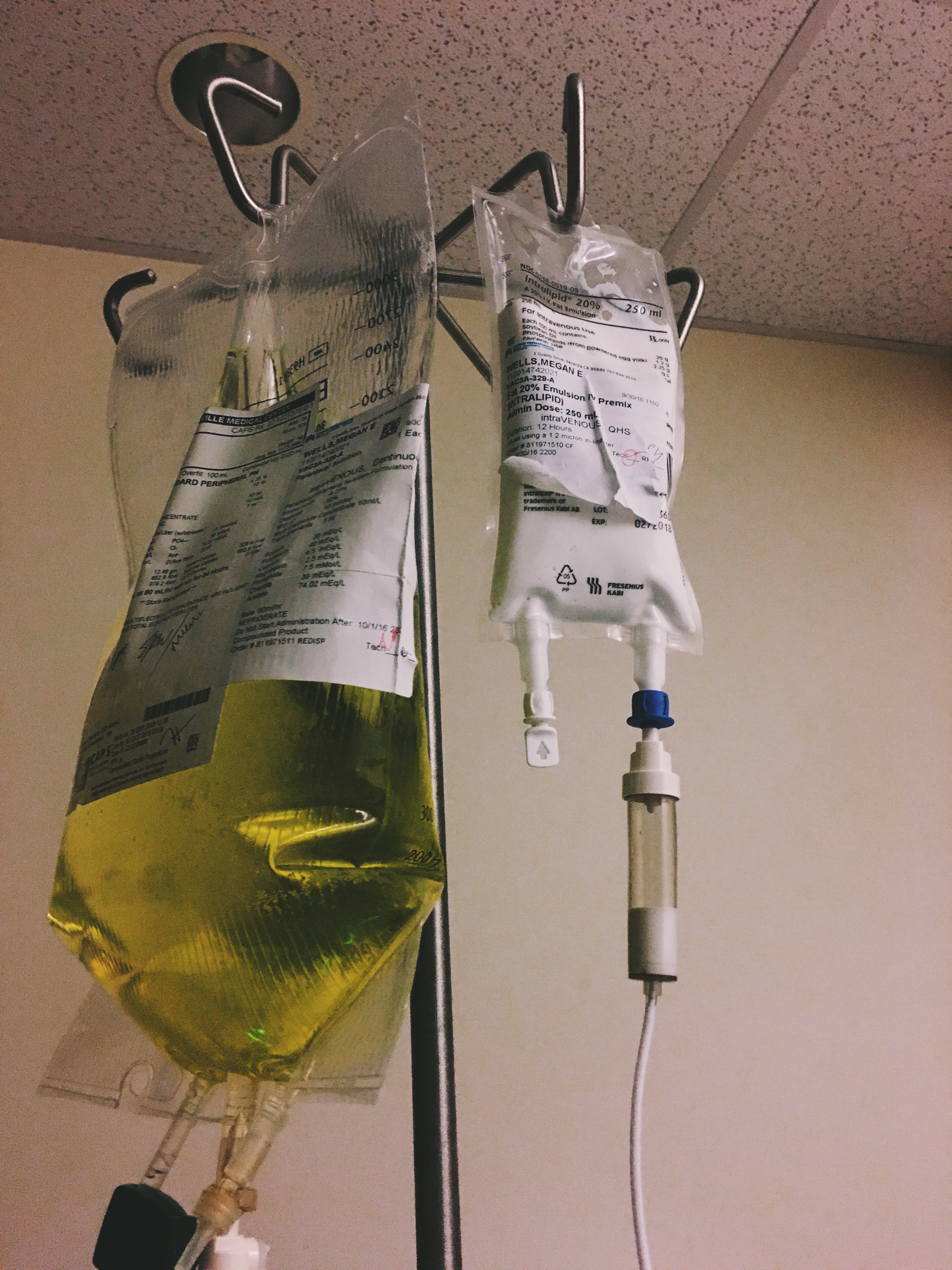
By Wednesday the 28th, I felt well enough to update everyone on Facebook. That task was made easier by the fact that the first IV site in the crook of my arm failed.
When IVs are in the crook of the arm, you have to try your best to keep your arm straight. Even a slight bend while texting can eventually bend the needle and make the IV site stop working.
That site was replaced with two more IVs on the same arm. One IV was for fluids and medicine while the other was for IV nutrition. All the doctors were very concerned about my weight and malnutrition.
IV Nutrition Complications
Throughout the rest of my stay, keeping me attached to the IV nutrition line was a big priority. But IV nutrition is extremely hard on the veins and IV site, so clogging, swelling, and leaking happens.
Eventually one of my arms began to look like Popeye’s because it became swollen and lumpy. And both of my arms started to hurt quite a bit.
Nurses had to play a round of musical chairs with all my IV sites, switching them, giving me new ones, and taking out ones that were too infiltrated. ICU nurses had to be called in to in to mine my veins, using AccuVein and ultrasound machines.
Many nurses told me I should heavily advocate for a peripherally inserted central catheter (PICC) line, which would help reduce the frequent needle sticks and vein irritation. But doctors didn’t think it was necessary.
Endoscopy, Tuesday September 29th
My throat started to hurt really bad from the NG tube and talking was hard. My mom brought a dry erase board for me so that I wouldn’t have to talk as much.
I had the NG tube in for three days and it pumped 3,500 mL of liquid out of me. The color started off rust-brown but eventually changed to a deep red color.
My mom thought it was blood and pointed that out to my nurses. But none of them took her seriously and kept brushing her off.
To be fair, earlier a nurse had changed the tube and it turned out the fluid was clear but it kept getting stained by what had passed through before. But once the new tube turned a deep red color, my mom raised her concerns again.
Finally, on Tuesday, when my GI doctor came to look in on me, she looked at the fluid coming out of the tube and her eyes got really big. She practically screamed, “That’s blood!
On her orders, it was removed right away and an hour later she performed an endoscopy on me. I hadn’t had an endoscopy since I was first diagnosed with ulcerative colitis in 2014.
Ulcers
Surprisingly, the endoscopy showed that I had old ulcers in my stomach that were almost all healed up. So, ulcers had been a problem for me at some point but I hadn’t even known it. There were also new bleeding ulcers, likely caused by the NG tube.
The medicine cocktail they used to knock me out kept me blissfully out of pain for a while. I thought maybe ulcers didn’t hurt too bad comparatively to everything else going on with me.
After waking up from a nap though, I did one walk around the floor and realized all the meds had finally worn off. Ulcers hurt.

Once the NG tube was removed, I began to feel a lot better. I wasn’t needing pain meds as much, I was allowed to eat ice cubes, and I was able to interact with my nurses.
With the NG tube in, I couldn’t communicate with my nurses very well and the tape hides your features, making it harder for people to connect with you.
The nurses didn’t treat me badly, I was still given the same treatment as everyone else. But they didn’t really see me as a person.
As soon as I was able to start talking to them and making connections, my hospital stay became better and I felt human again. When you are unable to talk and communicate properly, you feel like a piece of meat.
Getting Antsy, Impatient, and Frustrated, October 1st
By October 1st, I was beginning to get antsy and impatient. Overall, this was a good sign. It meant that I was feeling a lot better and my pain was no longer overwhelming all of my other senses.
But I was still not well enough to go home. My doctors and nurses knew it. And I knew it too, but that didn’t stop me from feeling trapped.
The hive like rashes across my neck from the opiates began to bleed from rubbing against my hospital gown ties and they became bed sores. My pillow was dotted with blood stains. My skin, especially my hands, were extremely dry and cracked, which added to the antsy feeling.
I hadn’t had another x-ray since the beginning of my hospital stay, so they did another to see if I could advance to a pureed diet rather than a full liquid diet.
A full liquid diet is extremely rich and has never sat well with me, so I asked about trying a pureed diet instead.
The x-rays showed that my intestines still had dilated loops, which brought my hopes down. I wanted to graduate to the next stage so badly and get home.
One GI doctor mentioned that sometimes the intestines never recover, and the dilation can be permanent. This snuck into my mind and I began to worry that that would be my fate.
Deep Vein Thrombosis (DVT), October 4th
From October 1st through the 4th, not much else happened. The days were monotonous and boring. I moved from a clear liquid diet, to a pureed diet, and to solids successfully. Normally, I’d be good to go home. But another complication cropped up.
The arm that was being used to give me nutritional IV fluids and lipids was becoming more swollen and painful every day. On October 3rd, I was tested for blood clots with an ultra sound but only superficial blood clots were found.
Superficial blood clots don’t need treatment. If they come loose, they don’t lead to a heart attack, stroke, or pulmonary embolism.
But on October 4th, I woke up and my arm was worse. My hand was blue-grey and the whole arm was swollen. My nurse took the IV out immediately. At the time, I was attached to the lipid IV nutrition, which is white and very thick.
When the IV was taken out, white fluid started leaking out of my arm. It smelt like a mixture of milk and vinegar. It was very surreal seeing fluid that wasn’t blood leaking out of my arm.
I was sent off for another ultrasound and this time, since the IV was removed, my whole arm was scanned. And towards my wrist, they found a deeper blood clot, or deep vein thrombosis (DVT), that would require treatment with blood thinners.
Getting educated about blood thinner medication
Because of this, I couldn’t be discharged. I had to wait until the next day for a nurse to come by and educate me on the blood thinner medications I would have to take. This included self-administered shots for a couple of weeks and Coumadin for six months.
I’ve never had to take such a complicated medication before. Blood thinners interact with a lot of vitamins and foods. They are also very sensitive to your body’s chemistry. It requires constant adjustments to doses, which is figured out from various blood tests done every couple of weeks.
Discharge, Wednesday October 5th
After I got educated on blood thinner medication, I was finally discharged from the hospital. I’ve never been so happy to be discharged in my life. I felt like if I didn’t get out soon, something else would go wrong and I would never leave.
Yes, it’s possible to die from ulcerative colitis
There are a couple of conclusions that I came to during this time. One of them being that it is possible to die of complications from ulcerative colitis.
In the past, every single time I had a flare I was always able to recover fully before the next one. It sucked that I kept having flares and had to be hospitalized every year. But I always had a six month to year break between hospitalizations.
That was long enough to almost heal completely and feel healthy again before going through the same cycle again. This was my first time that I didn’t have time to heal.
One of the nurses I had was asking really intelligent questions about ulcerative colitis. They were the type of questions that made me think he either had ulcerative colitis or knew someone close to him that had it.
And sure enough, he told me he was an ambassador to the Crohn’s and Colitis Foundation. He said, “I had a friend…well maybe I shouldn’t tell you.”
I said to go ahead. So, he continued.
“Well, he actually died of complications from ulcerative colitis. He died of pneumonia. But this was a long time ago and treatment wasn’t as good as it is now.”
my nurse
I told him that I believed him. Because the way it stands now, if this happens to me again, without more time to recover, it’s going to be really bad.
Feeling the specter of death
My body doesn’t have enough reserves, enough strength, enough anything really to defend itself. If I caught hospitalized-acquired pneumonia, which is completely possible considering how long I was hospitalized, I might die.
And even if I managed to not die, the probability of coming out of the ordeal with even worse consequences is high. This time I came away with some consequences outside of the usual. So now I understand how death is possible.
Every time you go through a health trauma, you learn something new about your disease, about how your body functions, and about how much your body can endure.
This time I learned there is a limit to what your body can endure. And that’s why I’m scared. I can’t have anything else go wrong. If I was in a video game, one more hit would kill me.
Weaknesses in the medical care system
I’ve learned a lot about my body and the medical care system. And I think there were two factors that made my quality of care not be as good as it could have been.
The first is how specialized my body and medical history is. It’s literally a novel now. There is so much there and I don’t have a normal functioning body.
The second is my age. A lot of what I’ve gone through is normally only seen in elderly populations.
Having a specialized body
There was a high amount of specialty care that went into my surgery and into making my body work. So as a result, there are only a small amount of people in the hierarchy of medical professionals that really get me.
I can’t recall how many times a nurse or doctor on the floor was examining me and thought my j-pouch was on the outside of my body.
The first time I was in the hospital with post-operative ileus, I didn’t have a GI doctor or colorectal surgeon looking after me. They weren’t contacted or updated on my condition.
Only surgeons who had a general idea of the procedure were on my case. And they readily admitted that they didn’t know how my j-pouch was supposed to be functioning or how I was supposed to be feeling.
When I was released the first time for post-operative ileus, I spent a week and a half in a lot of pain. I had to force myself to eat and it was very painful going to the bathroom. It felt like a really bad ulcerative colitis flare.
But I didn’t know how I was supposed to feel. I did some research online and read what other people experienced after the same procedure. And it seemed like cramping and pain while going to the bathroom was common. So, I started thinking that maybe I was a wimp and needed to just suck it up.
Your surgeon is part of your team for life
At this point I should have contacted my surgeon and told him what I was feeling. But I didn’t. I still had the mindset that my surgeon was no longer part of my medical team.
But now I’ve learned, anytime I think something is going wrong or I have a question, there are two people I need to contact: my GI doctor and my surgeon. Because they’re going to have to work together to figure out what the heck is going on.
Because that’s what happened the second time around. I had a whole team made up of the doctor on call, a GI doctor, and a surgeon come into my room all together to discuss my condition and progress. And they made sure to continually update my surgeon.
And everything went a lot better the second time around. People who have more specialized knowledge were on my case and could make better decisions about my condition.
My Age
Another reason I was discharged too early the first time around is that I’m young. A lot of people who go through this surgery are older. And older people are treated with more care because they are more fragile.
When you’re young like me, medical professionals tend to be a little more cavalier. I felt like the attitude was “you’re young, you’ll get over it.”
But during my second hospitalization for post-operative ileus, everyone started paying more attention.
Every shift change, nurses go over your history and the reason why you are hospitalized. It’s a little different every time, almost a little like telephone. Some details get murky and twisted or other times a nurse will focus on other parts of your medical history.
But the last time, all my nurses’ eyes got really big when reviewing my chart. Because by that time, it was my fourth hospitalization in two and a half months. Overall, I was almost in the hospital for a full month. And that raises some eyebrows no matter what age you are.
I’m not a healthy young adult
My weight also made medical professionals pay more attention to my case. I was weighing in around 95 pounds and my blood work showed that I was extremely malnourished.
All these factors built up to make them pay attention. And it’s not like they weren’t paying attention before, but they were treating me like a healthy young adult who happened to have surgery.
And I’m not a healthy young adult. I’m a young adult, but everything else is not true. I’m not healthy, or I wasn’t at the time and I had a very specific case history.
This time they were very alert to the fact that I was not a healthy young adult and they handled me with gloves.
My Body Now

My body after this whole ordeal.
- Weight: 95 pounds
- The dots are from all the blood thinner shots I have to take for blood clots
- The scar near my belly button is where my stoma was
- All the rest are from the first surgery where they removed my colon
I’m doing great now. Eating is easy and there is no pain involved. I’m still having to figure out what I can eat with my new system but it’s not so scary now. At the end of three months, I’m hoping I’ll be able to eat anything I want.
My goals include
- Gaining 20 pounds
- Start lifting weights and doing yoga to help get some muscle mass back
- Start running again (once I’ve gained some weight back)
Recovering from Pain and Standing in the Sun
Your pain is the breaking of the shell that encloses your understanding. Even as the stone of the fruit must break, that its heart may stand in the sun, so must you know pain.
kahill gibran, the prophet, on pain
Kahill Gibran’s beautiful words have never reverberated more with me than at this moment in time.
The past two and a half months have been the worst in my life. I had no break from my pain, no time to recover from my battles and wounds, and no time to hope for the light at the end of the tunnel.
So many emotions
Now that I’ve escaped from the hospital and am doing well, I find myself extremely emotional at times. This weight of emotion is usually triggered by music like
- A very beautiful cover of Landslide
- Unsteady by the X Ambassadors
I want to start crying but it’s not from sadness. It’s from an incredibly strong feeling of gratefulness and relief that I haven’t had more complications. That the cycle of pain is over.
And the reason Gibran’s words come back to me is that I have to find some warmth and positivity in what happened to me.
I’ve shed another layer of the shell that encloses the seeds of understanding, compassion, and empathy. Now that I’m free, I’m able to grow and stand in the light of the sun, enlightened by my experience.
That’s what I take from pain. That’s what I learn from pain. And I’m grateful. Because I could learn bitterness or hate.
Just know that all of you, through Facebook comments, texts, and calls, have shined some light into my darkness. I’ve learned people have so much compassion. And that’s beautiful.
What’s next on the blog
I’m well enough now that I want to start posting again. I have a whole bunch of cookie recipes that I’ll start sharing.
I’m really bummed that I missed the whole Halloween and Thanksgiving food blogger period. But next year. And I still might be able to fit in a Thanksgiving pie or something.
Facebook Live Video Updates
When I was going through this, creating a blog post was too hard for me. All the information in this post was compiled from the Facebook updates I posted while in the hospital and from these live video updates.
My Whole UC Story
You can read my ulcerative colitis story in order or you can browse all my ulcerative colitis and health-related posts here:
- My UC Story: where and when my ulcerative colitis symptoms first started
- Part I – The Beginning of My UC Story: what my symptoms were and the struggles I had getting health care
- Part II – UC Diagnosis and Adjustment: how I was diagnosed and how I struggled to adjust to living with ulcerative colitis (including diet experiments, and getting frustrated with doctors not listening to me)
- Part III – UC and Severe Back Pain: my ongoing struggle with severe back pain + getting a new GI doctor that listened to me and who sent me to a rheumatologist
- Part IV – Sacroiliitis Diagnosis and UC Remission: getting diagnosed with sacroiliitis, getting on Remicade, and finally going into remission (with both my UC and joint disease)
- Part V – The Second UC Flare: my slowly deteriorating health, worsening symptoms, colonoscopy, and my first ER visit
- Part VI – First Hospitalization: my first hospitalization from my second ulcerative colitis flare and my experience with bowel rest and edema (swelling from fluid).
- Part VII – Being on Prednisone for My Second UC Flare Recovery: being on Prednisone for the first time and the various effects it had on my mind and body + adding mercaptopurine (6MP) and allopurinol to my daily routine
- Part VIII – Third UC Flare and Second ER Visit: my third UC Flare experience, symptoms, ER visit, and tests and procedures (CT scan, proctoscopy, etc.)
- Part IX – Recovering From Two Consecutive Flares: being released from the ER and the struggles of recovering from two consecutive UC flares (three months apart)
- UC Planning Realities: Trying to Write and Defend a Thesis: the difficulties in making long-term plans with UC and trying to meet thesis deadlines while in a flare
- Post UC Flare Routine: my post UC flare routine that helped me manage my physical and emotional symptoms
- Body Image and Mental Health with UC: Stop telling me I look great: the connection between body image and mental health and how my experience with ulcerative colitis has complicated my relationship with the two
- Making Travel Plans with UC: the difficulties in making travel plans with UC
- The Nightmare of Ulcerative Colitis: I compare a reoccurring childhood nightmare I had to the nightmare of ulcerative colitis
- Part X – Fourth UC Flare: My fourth UC flare experience, symptoms, hospitalization, tests, procedures, next treatment steps, and recovery
- Hanging Out in Limbo: waiting for experts to weigh in on my situation is like hanging out in limbo – I have no new treatment plan and I don’t know what the future holds
- Part XI – How Losing My Colon is a Transformation and Not a Loss: I’m losing my colon soon. But read about how this is a transformation and not a loss and how I made the decision to remove my colon
- You’ve Just Crossed Over into the Prednisone: Being on prednisone is a lot like being in the Twilight Zone. Things aren’t always what they seem, it can be hard to navigate and understand your surroundings, and often times you feel like you might never come back. Or the even scarier thought: that you might not ever want to come back.
- Recovery Reads: a list of some of my favorite books to read while recovering from UC flares, hospitalizations, and surgeries
- Pre-Surgery Jitters: my pre-surgery jitters in the days leading up to my j-pouch surgery on May 20, 2016, and how I distracted and pampered myself
- Part XII – J-Pouch Surgery: what my j-pouch surgery (proctocolectomy with ileal pouch-anal anastomosis) was like, including prep, surgery, and recovery
- J-Pouch Surgery Recovery: j-pouch surgery recovery is a full-time job with lots of road bumps along the way including bladder problems, dehydration, exhaustion, healing stitches and scars, pain and emotions, and adjusting to life with a stoma and ostomy bag
- Stoma Life: what my stoma life, the three months I lived with an ostomy bag, was like, including the physical and mental adjustments I went through, procedures, and what travel was like
- Part XIII – Pancreatitis: my struggle with pancreatitis including symptoms, tests, my ER and hospital stay, pain management, post-discharge recovery, and pre-op prep
- Part XIV – Ileostomy Takedown Surgery: how my ileostomy takedown surgery went, including prep, the surgery, hospital recovery, and complications
- Part XV – Post Operative Ileus Complications: my painful and scary experience with post operative ileus complications left me very weak, under 100 pounds, malnourished, and very close to death’s door
- Surgery Recovery and Diet Problems: Physical and diet difficulties from post-surgery recovery and complications from pancreatitis, post-operative ileus, and pouchitis
- Everything is Shiny and New
- Hitting the Wall and The Privilege of Scars and Wrinkles
- Experiencing Loss and The Power and Comfort of Creativity
- Hauntings, Superstitions, and Giving Back: Reflecting on Being Hospital Free for 2 Years
Oh man, you poor thing!! I’ve seen you around some of the FB sharing groups, but I haven’t visited your site for a while and this is my first time hearing about all this. I hope that the worst is over and you are on the mend now. 🙁
Thank you so much for your kind words Natasha! I’m doing so much better now and the whole horrible ordeal is over.
Oh my word girl! I missed a lot of this. I’m so glad you’re out of the hospital and back home!! Heal up! I’d been wondering how you were doing.
Oh-And you could totally still do fall food- it’s not even November yet! 😉
Ah thanks so much Sarah! It’s so good to hear from you and to be back in the swing of things.